13yo left testicular torsion resulting in orchiectomy
Case Overview
- FL
- 13 years old, Male
- None listed
A 13-year-old male with no chronic conditions documented in the available records and no known drug allergies presented on Day 1 to an emergency department with lower abdominal/suprapubic pain that began at approximately 10:00 p.m. the prior evening, associated with nausea and a “pee sensation, no pee” history reflected in the review materials. Past surgical history later documented circumcision in 2023; otherwise history was described as unremarkable. Home medication history included ibuprofen 600 mg PO every 6 hours as needed for pain from a prior encounter. The primary specialty for review is Emergency Medicine, focused on evaluation of an adolescent male with acute lower abdominal/suprapubic pain and the subsequent diagnosis of left testicular torsion with loss of the left testicle.
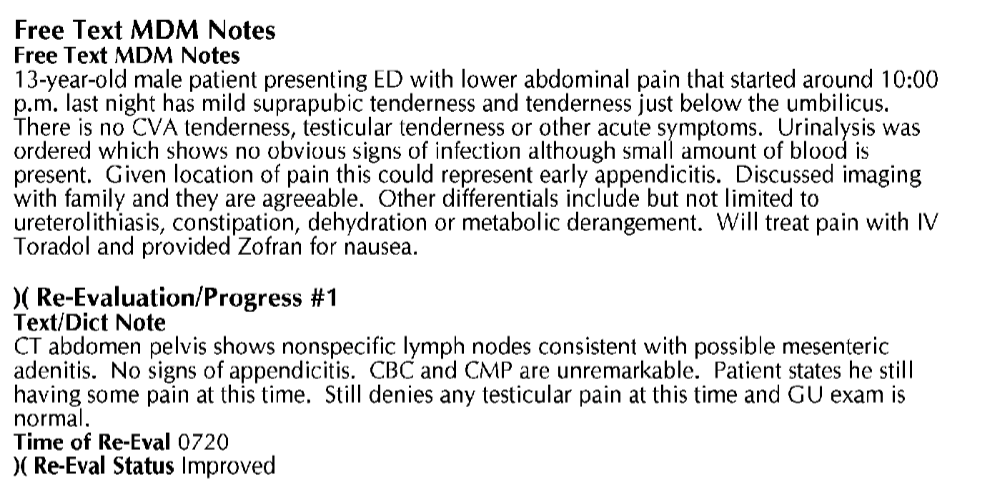
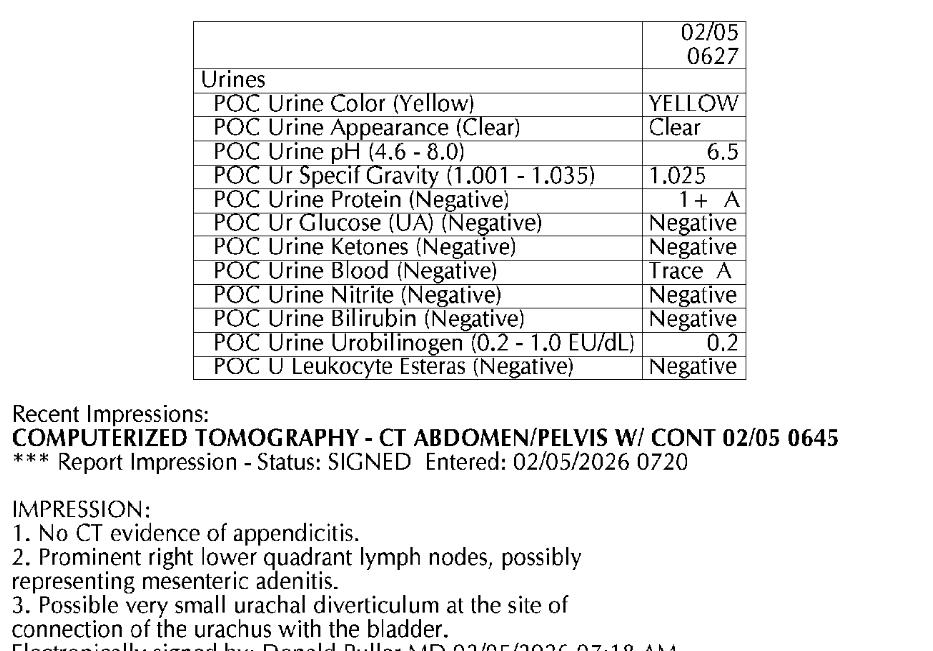
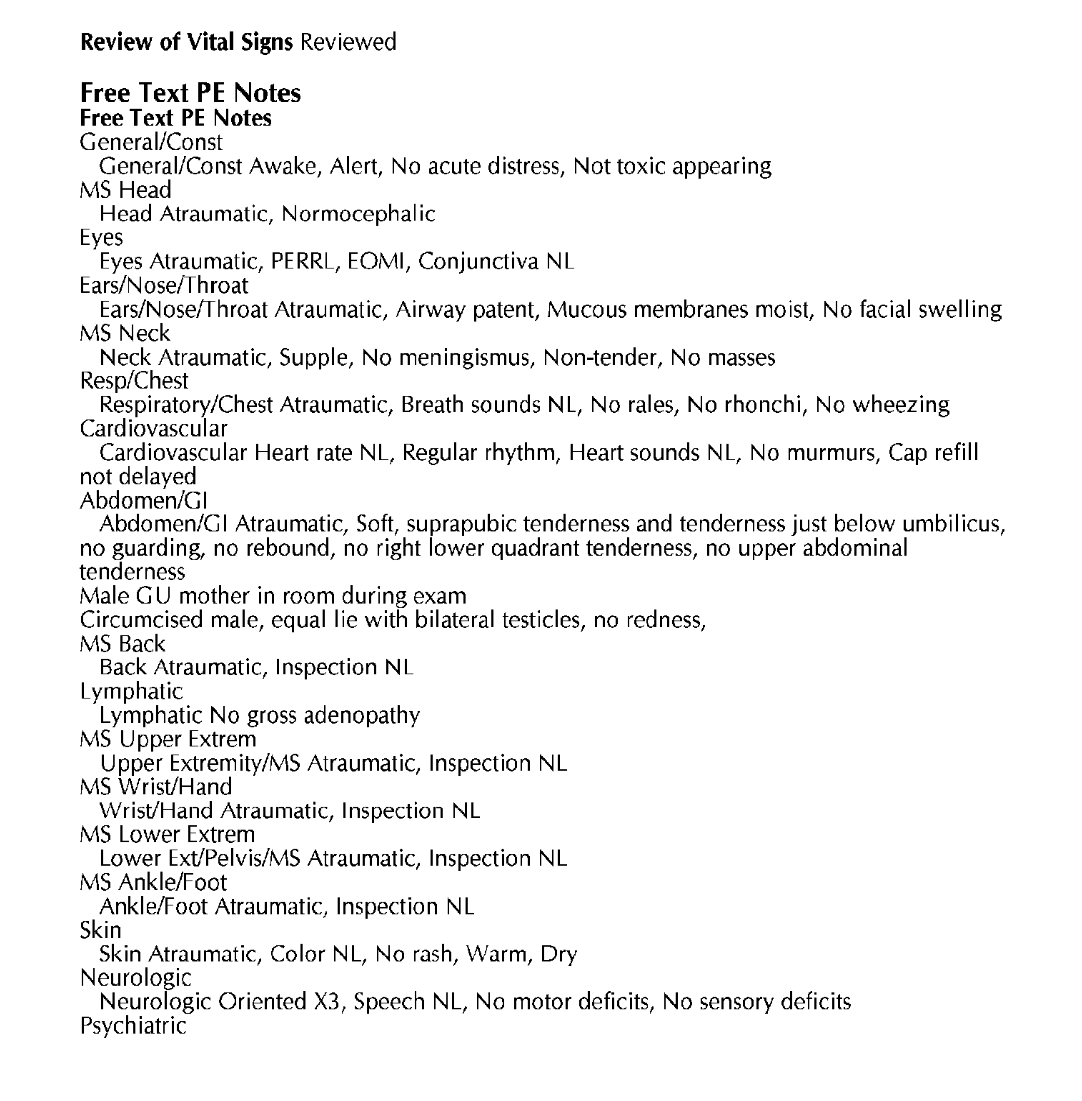
On Day 1, the emergency record documented a 13-year-old male with lower abdominal pain, mild suprapubic tenderness, and tenderness just below the umbilicus, with no CVA tenderness and documentation stating no testicular tenderness or other acute symptoms. Urinalysis reportedly showed no obvious infection with a small amount of blood; CBC and CMP were described as unremarkable. CT abdomen/pelvis with IV contrast was ordered at approximately 6:42 a.m. to rule out appendicitis and reportedly showed nonspecific lymph nodes consistent with possible mesenteric adenitis and no appendicitis. Medications included ketorolac 15 mg IV ordered at 6:42 a.m. and administered at 6:51 a.m.; acetaminophen 1,000 mg PO and dicyclomine 20 mg PO were ordered at 7:25 a.m. and administered at 7:26 a.m.
At re-evaluation around 7:20 a.m., the patient still had some pain but was improved; the record states he still denied testicular pain and that the GU exam was normal, though the available excerpts do not provide detailed scrotal exam elements such as lie, cremasteric reflex, swelling, erythema, or palpation findings. There was no scrotal ultrasound ordered or performed, nor any consult with urology.
**Please see attached chart screenshots for reference**
On Day 4 at 10:51 p.m., he returned with groin pain “x Thursday,” fever, testicular pain, and testicular swelling; initial vital signs were BP 132/62, HR 103, RR 16, temperature 37.0°C, SpO2 97% on room air. The treating clinician documented suprapubic abdominal pain, nausea, and bilateral testicular pain; on exam both testicles were exquisitely tender, firm, edematous, and erythematous, and a stat scrotal ultrasound was ordered. Acetaminophen 1,000 mg PO and ibuprofen 600 mg PO were ordered at 11:04 p.m.; ibuprofen was administered at 11:15 p.m. Scrotal Doppler ultrasound performed late Day 4/early Day 5 showed right testicle 3.8 x 2.0 x 2.4 cm with normal vascularity and left testicle 3.5 x 2.7 x 3.0 cm with heterogeneous appearance and absent vascularity, suggestive of torsion.
After the absence of left testicular blood flow was identified, the record reflects immediate transfer-center contact for pediatric urology; the patient was accepted by a pediatric receiving facility, and transport picked him up at 1:45 a.m. on Day 5. Transfer vital signs just prior to transfer were documented as temperature 98.3°F, pulse 62, respirations 14, BP 141 systolic with the diastolic value not clearly visible in the excerpt, and SpO2 100%. He arrived at the receiving emergency department at 2:14 a.m. on Day 5, weight 80.4 kg; fentanyl 50 mcg IV was ordered at 2:16 a.m. The receiving emergency record documented ultrasound-confirmed left torsion, physical exam concerning for torsion, and discussion with urology at 2:17 a.m.; urology was en route and planned operative evaluation. Urology consultation at 2:51 a.m. documented vital signs temperature 97.7°F, pulse 87, BP 129/85, RR 20; abdomen soft, nontender, nondistended; GU exam showed circumcised normal meatus, testes descended bilaterally without nodules, and left hemiscrotum erythematous and edematous with a firm, tender testicle. Surgery occurred approximately 3:16–3:44 a.m. on Day 5 and included scrotal exploration, left orchiectomy, and right testicular fixation under general endotracheal anesthesia.
Operative findings were left testicular torsion with necrotic left testicle, no bleeding upon incision of the tunica albuginea, and necrotic seminiferous tubules; estimated blood loss was less than 5 mL and complications were documented as none. Surgical pathology of the left testicle showed testicular tissue with marked interstitial hemorrhage and infarction, consistent with clinical history of torsion; gross description included a 30 g, 4 x 3 x 3 cm testicle with a 4.5 cm x 1.5 cm spermatic cord segment, purple-red tunica vaginalis, diffusely soft hemorrhagic parenchyma, and hemorrhagic epididymis, with no lesions identified.
1. In a 13-year-old male presenting on Day 1 with acute lower abdominal/suprapubic pain and nausea, did the Emergency Medicine standard of care require performance and documentation of a detailed genitourinary/scrotal examination as part of the initial evaluation (possibly including a SWFIT score)?
2. Given the Day 1 presentation, including lower abdominal/suprapubic pain, urinary sensation without urination, nausea, and the adolescent male age group, would a reasonably competent emergency clinician have performed a scrotal ultrasound and/or sought consult with urology to rule out torsion?
3. If testicular torsion had been identified and treated on Day 1 at or near the reported onset of symptoms, what would the expected probability of testicular salvage have been compared with the outcome documented after Day 4/Day 5 presentation?
4. Do the Day 5 operative findings of a necrotic left testicle and the Day 4/Day 5 Doppler finding of absent left testicular vascularity indicate that the testicle was likely nonviable for a period substantially longer than the Day 4 to Day 5 interval alone?
5. Is the Day 1 abdominal pain presentation, later characterized in the urology consultation as onset of left testicular pain with an earlier visit for lower abdominal pain, consistent with an early or developing testicular torsion presentation? 6. Does the Day 1 CT abdomen/pelvis provide any clinically meaningful findings, or lack of findings, regarding testicular perfusion or scrotal pathology?
Files:
Case Questions
No questions yet!
Want to open a case or submit response?

Comments are accepted only from Emergency Medicine - includes all subspecialties experts.